What Exactly Is A “G-Spot”?
Have you ever heard of the “G-Spot” and wondered what it is? Some people report experiencing orgasm and/or ejaculation and/or […]
What Exactly Is A “G-Spot”? Read More »
Have you ever heard of the “G-Spot” and wondered what it is? Some people report experiencing orgasm and/or ejaculation and/or […]
What Exactly Is A “G-Spot”? Read More »

Is Your Ovulation Boosting Your Man’s Testosterone Levels? I was speaking with a client from New Zealand last week, and
How Natural Ovulation May Boost Male Testosterone Levels Read More »
This month, I’ve decided to do a deep-dive into wearable skin temperature trackers. It’s my hope that this Info Hub
INFO HUB: Skin Wearables for Temperature Tracking Read More »

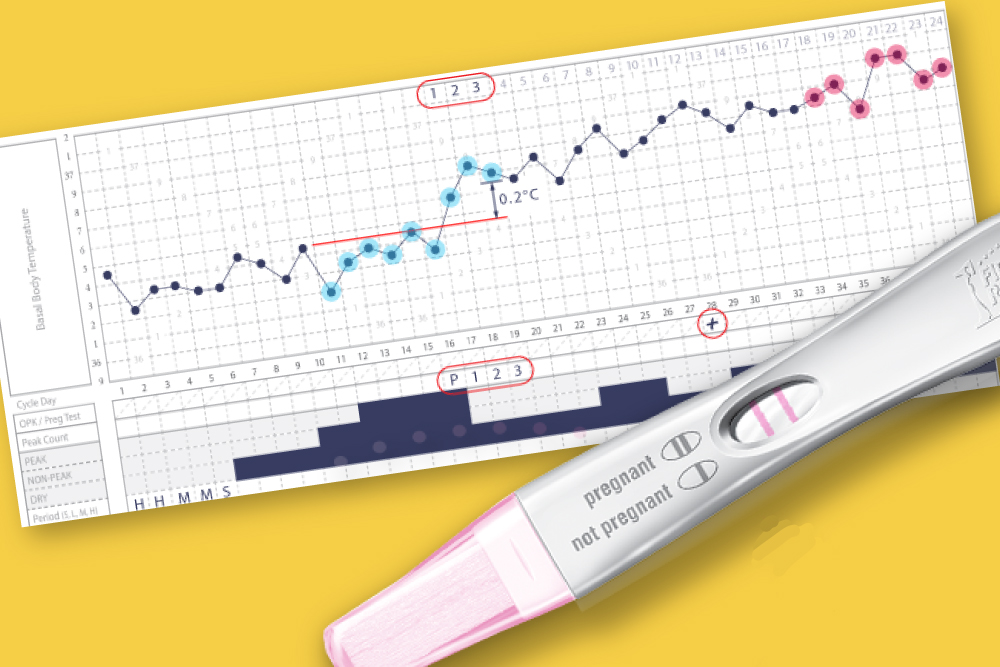
Without fail, one of the most common laments I hear is “I wish I had known about the Symptothermal Method
FABM Charting for Teens Read More »
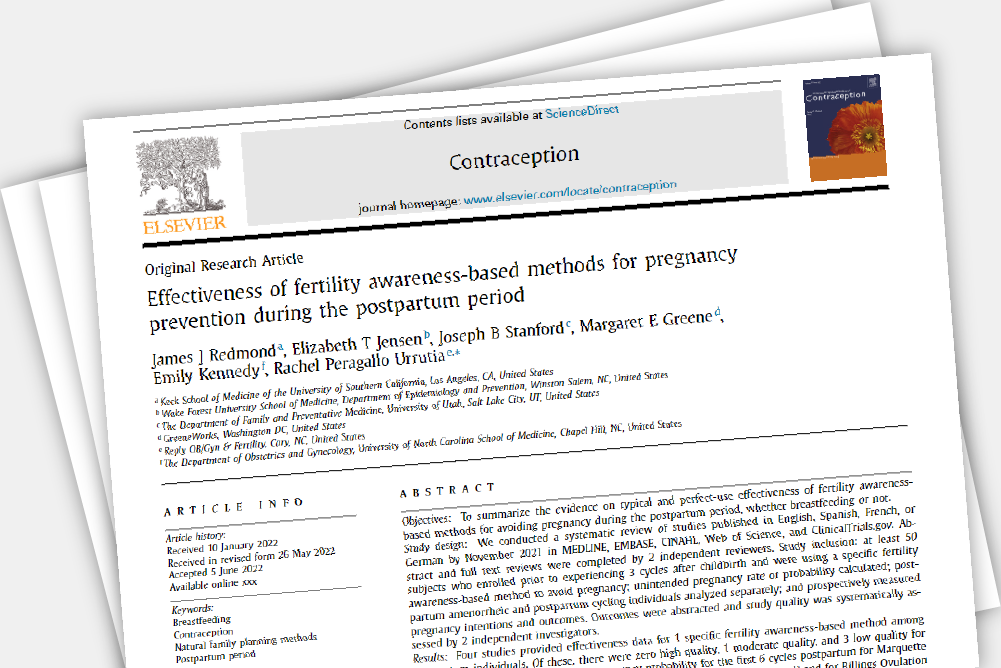
Disclaimer: I am writing this article from the depths of postpartum sleep deprivation. Please also keep in mind that I
FABMs in the Postpartum: Latest Systematic Review Read More »
When I first tell people that I teach clients how to chart their menstrual cycles to conceive, the initial reaction
Trying For A Baby? Why You Should Chart Your Cycles Read More »
Not a month goes by where I don’t get a question or a comment along the lines of “I’ve heard
Can the Moon Cause Random Ovulation? Read More »

Recently, The Guardian released an article titled “Women Don’t Need To Bleed: Why Many Women Are Giving Up On Periods”.
Your Menstrual Cycle Is More Than Just A Bleed Read More »

“My cycle would be one of the first indicators that it was time to slow down and engage in some
Meet the FABM: Rebecca McEvoy Read More »
THE SEX-ED YOU MISSED
Take the FREE Symptothermal Video Course to learn all about charting for birth control or to conceive.