Achieving a Pregnancy
THE FERTILITY AWARENESS ADVANTAGE
Each menstrual cycle provides a brief window of around six days of fertility. This takes into account the average lifespan of the sperm and the egg.
For couples who are not using the Symptothermal Method, general medical advice would recommend unprotected sex every 2-3 days throughout the menstrual cycle in hopes of lining up with the fertile window at some stage.
Many couples find that the advice of having sex every 2-3 days throughout the entire menstrual cycle can add undue stress and reduce the spontaneity of their sex lives.
Tracking cervical mucus and basal body temperature with the Symptothermal Method provides couples who are trying to conceive with the advantage of being able to time acts of unprotected sex to coincide with the fertile window. This can reduce the pressure to have sex every few days throughout the entire menstrual cycle.
Research is conflicting as to whether using Fertility Awareness-Based Methods to time sex to the fertile window can reduce the time it takes to fall pregnant. Some studies show a reduction in the time it takes to fall pregnant, while other studies show no difference in time to pregnancy between FABM users and non-FABM users.
While it’s plausible that there may be a small advantage for FABM users during the first few cycles of trying to conceive, by six months this likely disappears. In fact, at six months the conception rates between FABM and non-FABM users are very similar; 85% of couples have usually conceived by this time regardless of whether they are using a FABM or not.
Studies show that by 12 cycles of trying, between 82 – 92% of couples will have conceived. Those in the 30-39 year age bracket sit closer to 82%, while those in the 19-26 year age bracket sit closer to 92%

GETTING THE TIMING RIGHT
Using the Symptothermal Method helps us identify the opening and closing of the fertile window; however, the fertile window as identified by charting is often much longer than the actual biological fertile window (six days).
For this reason, it’s recommended to target unprotected sex to days when peak-type cervical mucus is present. Peak-type cervical mucus has a very high water content and provides ideal conditions for sperm survival and transport through the reproductive tract. Having unprotected sex on days with peak-type cervical mucus means that sperm have the best chance of surviving long enough to fertilise an egg.
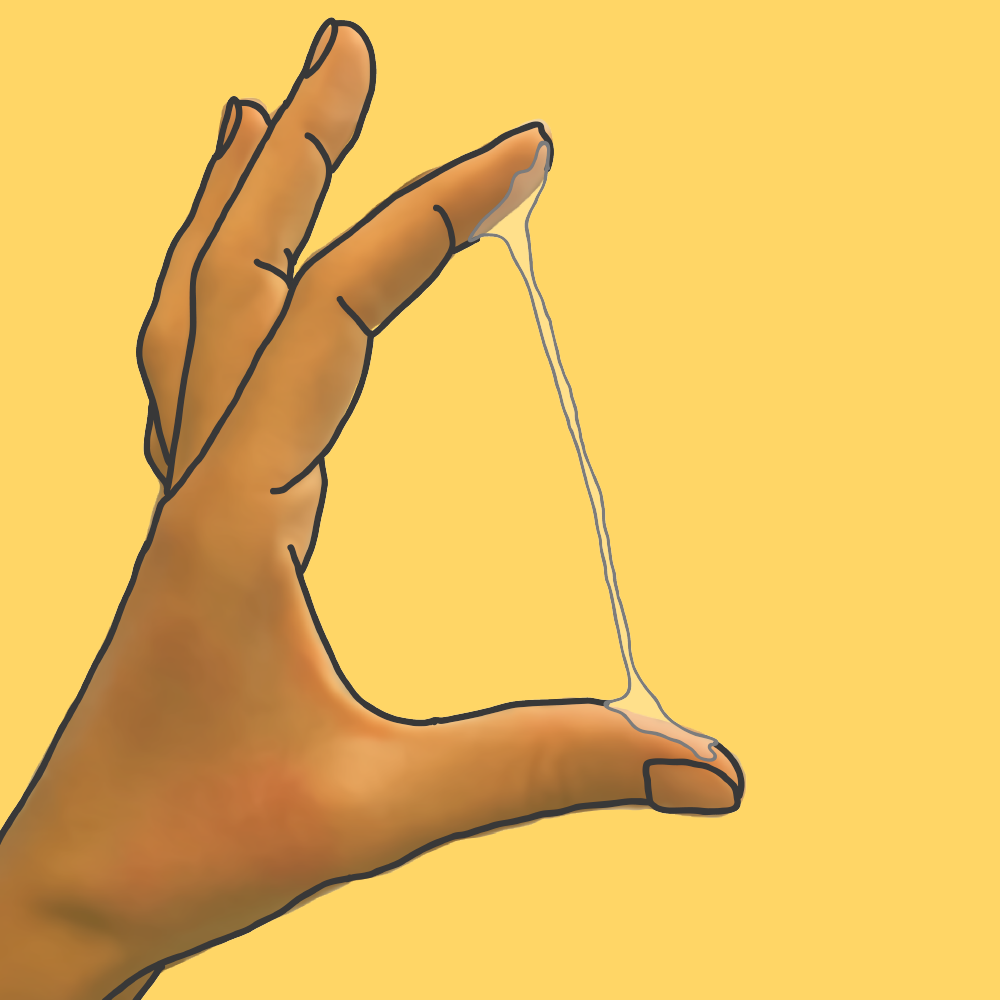
Remember, peak-type cervical mucus is usually associated with a lubricative vaginal sensation, and appears like raw eggwhite: clear, stretchy and slippery. Some people experience peak-type cervical mucus that has such a high water content that it is impossible to pick up or stretch. For women who don’t experience much cervical mucus at all, it becomes most important to focus on the vaginal sensation – a lubricative vaginal sensation is an important predictor of approaching ovulation.
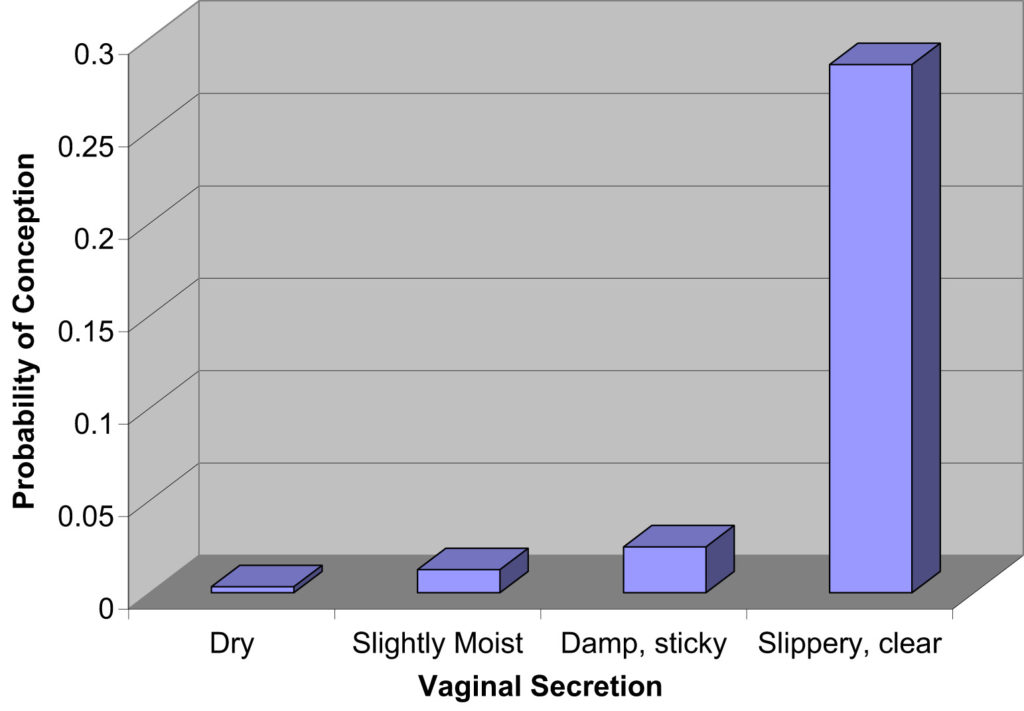
Studies show us that:
- The probability of conception is highest on days where clear, slippery and stretchy cervical mucus is present, and
- The probability of conception is highest on Peak Day and the two days before it.
It is recommended to have sex at least every 1-2 days during the fertile window, focusing especially on days where peak-type cervical mucus is present. Continue until the second day after the Peak Day, or the first day of the temperature shift; whichever occurs last.
The chances of conception are usually highest when sex occurs slightly in advance of ovulation. This allows sperm ample time to travel to the fallopian tubes where they can be ready and waiting for the egg to arrive. Sex on or after the day of ovulation may be less likely to result in pregnancy. This is because the egg itself only has an average lifespan of 17 hours, and many of the sperm spend up to 20 hours hibernating in the cervical crypts before proceeding toward the fallopian tubes.
Keep in mind that basal body temperature (BBT) holds no predictive value and cannot provide you with any warning that ovulation is approaching. Therefore, it’s most important to focus on observing your cervical mucus when trying to conceive. BBT is useful to confirm whether ovulation has occurred or not, and this can be helpful information for you on your TTC journey.
FREQUENCY: HOW MUCH IS TOO MUCH?
A widely held misconception is that daily ejaculation somehow weakens sperm or lessens the sperm count. Surprisingly, it has been proven that sperm concentration and motility remain normal, even with daily ejaculation (so there is no need to ‘save up’ sperm by postponing sex).
Interestingly, in men with a low sperm count, daily ejaculation may prove to increase sperm concentration and motility. In saying this, many couples would find daily sex during the fertile window a little stressful.
Best practice guidelines are to aim to have sex every 1-2 days during the fertile window, focusing especially on days where peak-type cervical mucus is present. Continue until the second day after the Peak Day, or the first day of the temperature shift; whichever occurs last.
LUBRICANTS
Most lubricants are damaging to sperm and can therefore negatively affect chances of conception. Saliva has been proven particularly damaging to sperm. If extra lubrication is needed, Pre-Seed lubricant has been studied and shown to be safe for sperm – it has not been shown to increase chances of conception but has at least been shown not to harm the chances of conception. Unfortunately, Pre-Seed contains parabens. If you want to reduce your exposure to parabens, I would recommend trying BabyDance lubricant instead. BabyDance lubricant has a similar sperm-friendly pH to Pre-Seed, but without the parabens.
Ideally though, the vaginal canal should be well lubricated during the most fertile days of the cycle due to the presence of peak-type cervical mucus. Where possible, it is best to take advantage of this natural lubrication and avoid introducing synthetic substances into the vagina when trying to concieve. We will cover strategies to promote healthy quantities of cervical mucus in Week 7.

WHEN AND HOW TO TEST
Home pregnancy tests measure the concentration of Human Chorionic Gonadotropin (hCG) in your urine. Remember that hCG is a hormone released by the developing placenta soon after implantation occurs.
In most successful pregnancies, implantation occurs around 8-10 days after ovulation. Levels of hCG usually reach high enough levels to provide a positive pregnancy test around 11-12 days after ovulation. It’s best to avoid testing any earlier than this to avoid the disappointment and emotional stress of a false negative.
For the purposes of counting 11-12 days from ovulation, you can assume that Peak Day was the day of ovulation. Although statistically ovulation could fall a few days either side of Peak Day, this is the closest marker that we can use to estimate the day of ovulation.

WHEN TO SEEK HELP
Unfortunately, not everyone who tries to conceive will fall pregnant straight away. Around 20% of couples who target unprotected sex to the fertile window using the Sympothermal Method will still be trying with no success at the six month mark.
If this is the case for you, it is recommended to seek out specialist evaluation and treatment after you have tried for six months (although the earlier the better as most specialists have long wait-times).
For couples who are not targeting unprotected sex with the Symptothermal Method, the usual advice is to seek out professional help after a full 12 months of trying.
POTENTIAL RED FLAGS
Charting your menstrual cycle with the Symptothermal Method provides you with a unique insight into your hormonal health. In Week 7 we will be discussing different ways that our charts might indicate issues that would be at odds with a healthy pregnancy.
PINPOINTING OVULATION (A MYTH)
A common mistake that new charters make, is thinking that the Symptothermal Method will somehow enable them to pinpoint the exact day of ovulation, which they can then use to try to conceive.
This assumption is unhelpful for two reasons.
- For the best chance of conception, sex should happen in advance of ovulation
- Charting does not help us to pinpoint ovulation, because we can never know in advance exactly when ovulation will occur.
The Symptothermal Method allows us to pinpoint the opening and the closing of the fertile window, but never the exact day of ovulation.
In fact, ovulation can occur on a wide range of days around the time of Peak Day and the temperature shift. A 1996 German study followed Symptothermal Method users with daily transvaginal ultrasounds and urinary LH tests. These results show when ovulation was occurring in comparison to Peak Day and temperature shifts:
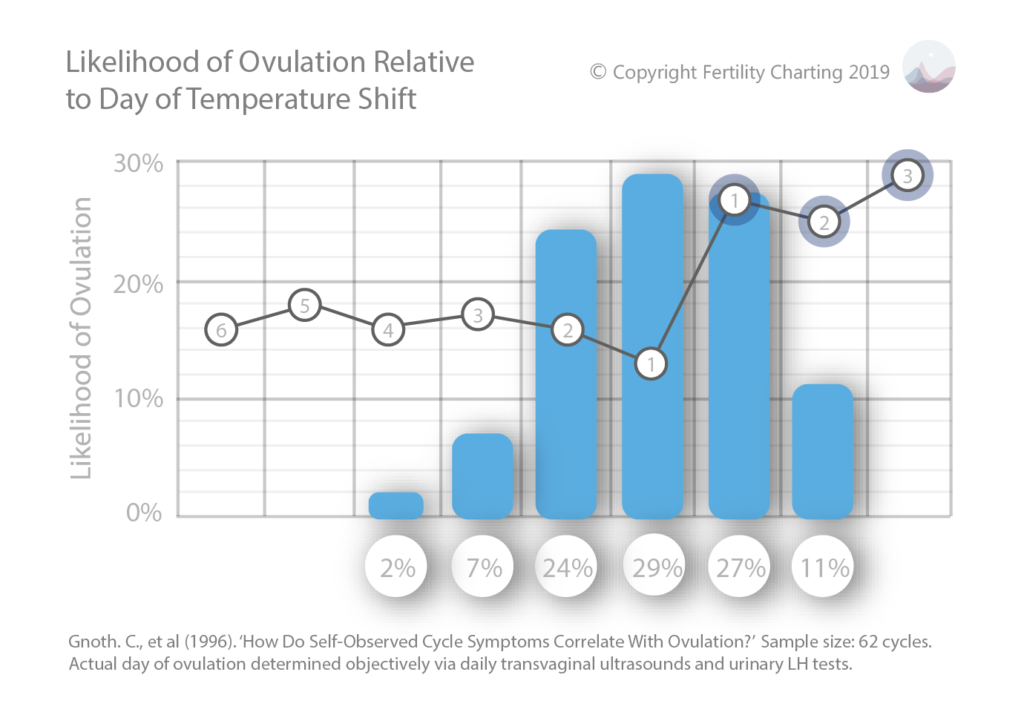
- Ovulation occurred the day before temp shift in 29% of cycles.
- Ovulation occurred on the same day as temp shift in 27% of cycles.
- Ovulation occurred two days before temp shift in 24% of cycles.
- Ovulation occurred on the second day of the temp shift in 11% of cycles.
- Ovulation occurred three days before temp shift in 7% of cycles.
- Ovulation occurred 4 days before temp shift in 2% of cycles.
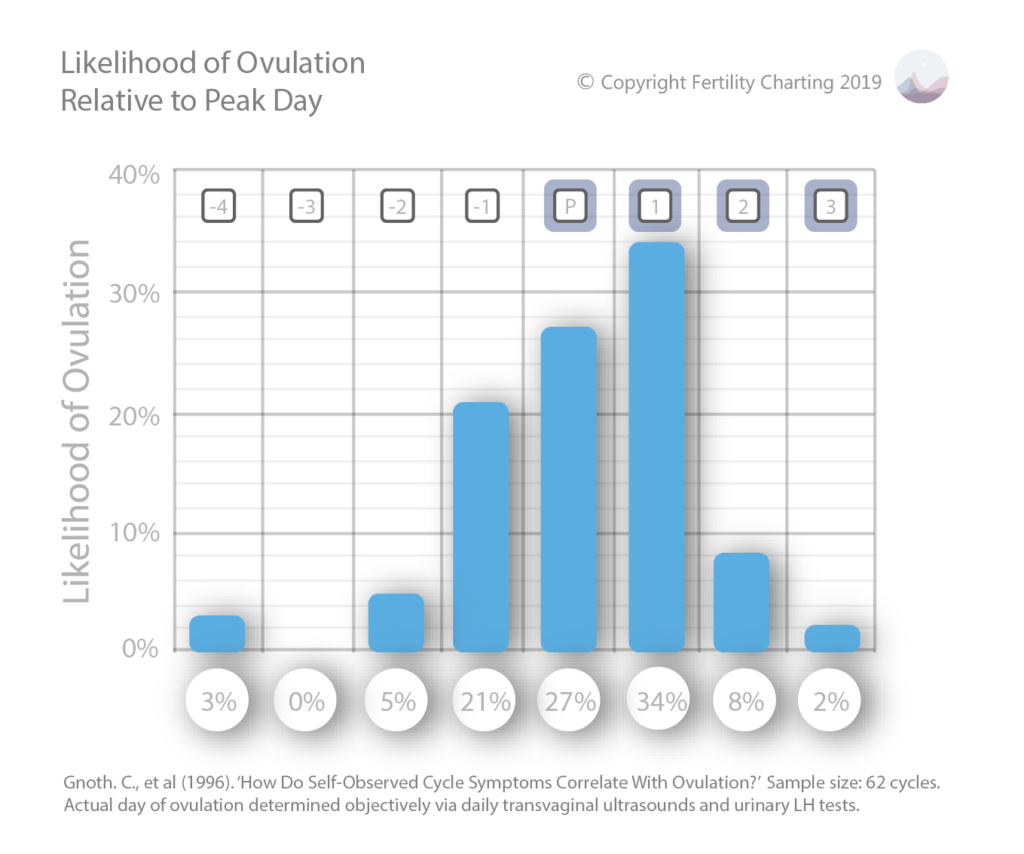
- Ovulation occurred on the day after Peak Day in 34% of cycles.
- Ovulation occurred on the day of Peak Day in 27% of cycles.
- Ovulation occurred the day before Peak Day in 21% of cycles.
- Ovulation occurred two days after Peak Day in 8% of cycles.
- Ovulation occurred four days before Peak Day in 3% of cycles.
- Ovulation occurred three days after Peak Day in 2% of cycles.
HOW TO CALCULATE YOUR DUE DATE
Once you confirm that you are pregnant, you will likely want to calculate your due date. A dating scan (ultrasound) in early pregnancy will provide the most accurate estimate of the gestational age of your baby (and therefore the estimated due date).
If you decline a dating scan, your doctor will likely calculate an estimated due date based on the first date of your last period. To do this, they simply add 280 days from the first day of your last period (based on the assumption that you always ovulate on day 14 of your menstrual cycle). Unfortunately, this can result in an inaccurate estimated due date, especially if you have very long cycles where you don’t ovulate until much later than cycle day 14. This can be problematic and in some cases can result in the induction of a premature baby.
Luckily, if you’ve been charting your cycles with the Symptothermal Method, you will have a much more accurate idea of when you have likely ovulated. You can assume that there will be 266 days between the first raised temperature and the estimated due date. Using the first day of your temperature shift, you can apply the below formula to calculate your estimated due date:
- Add nine months to the date of your first raised temperature
- Subtract one week (seven days) from that date
Whether you opt for a dating scan or use the above formula to calculate your estimated due date, it’s important to keep in mind that only around 5% of people actually give birth on their estimated due date. It may be more helpful to think of a “guess date” or a “guess month”.
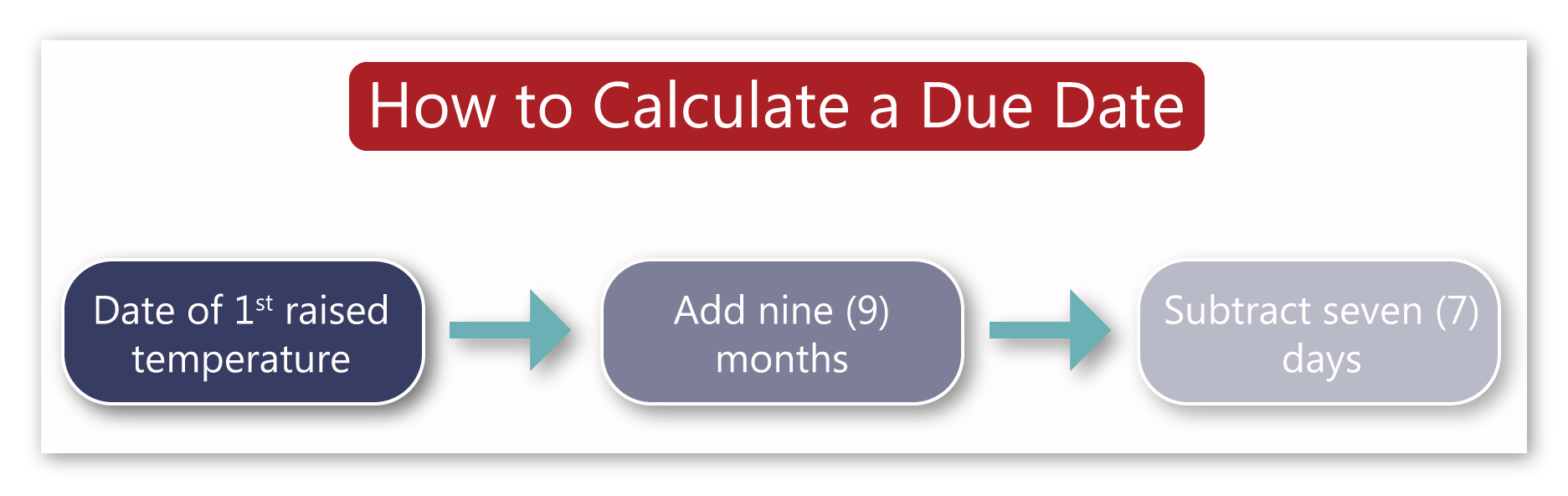
Example: Amelia is currently pregnant and has decided to calculate her due date. She checks her chart; the first date of her temperature shift was July 10th 2019. Amelia adds nine months which brings her to April 10th 2020. Amelia subtracts seven days which brings her to April 3rd 2020. This is the most accurate due date in the absence of an ultrasound.